
Meghanath Yenni: Key Takeaways From Updated NICE Blood Transfusion Guideline
Meghanath Yenni, Consultant Physician at Medicover Hospitals, shared a post on LinkedIn:
“Blood Transfusion: NICE Guideline (NG24, Updated 2026):
1. Core Principle:
- Use blood only when clearly indicated
- Prefer restrictive strategies
Always:
- Assess clinical status with labs
- Reassess after each unit/component
Aim:
Minimize unnecessary transfusions
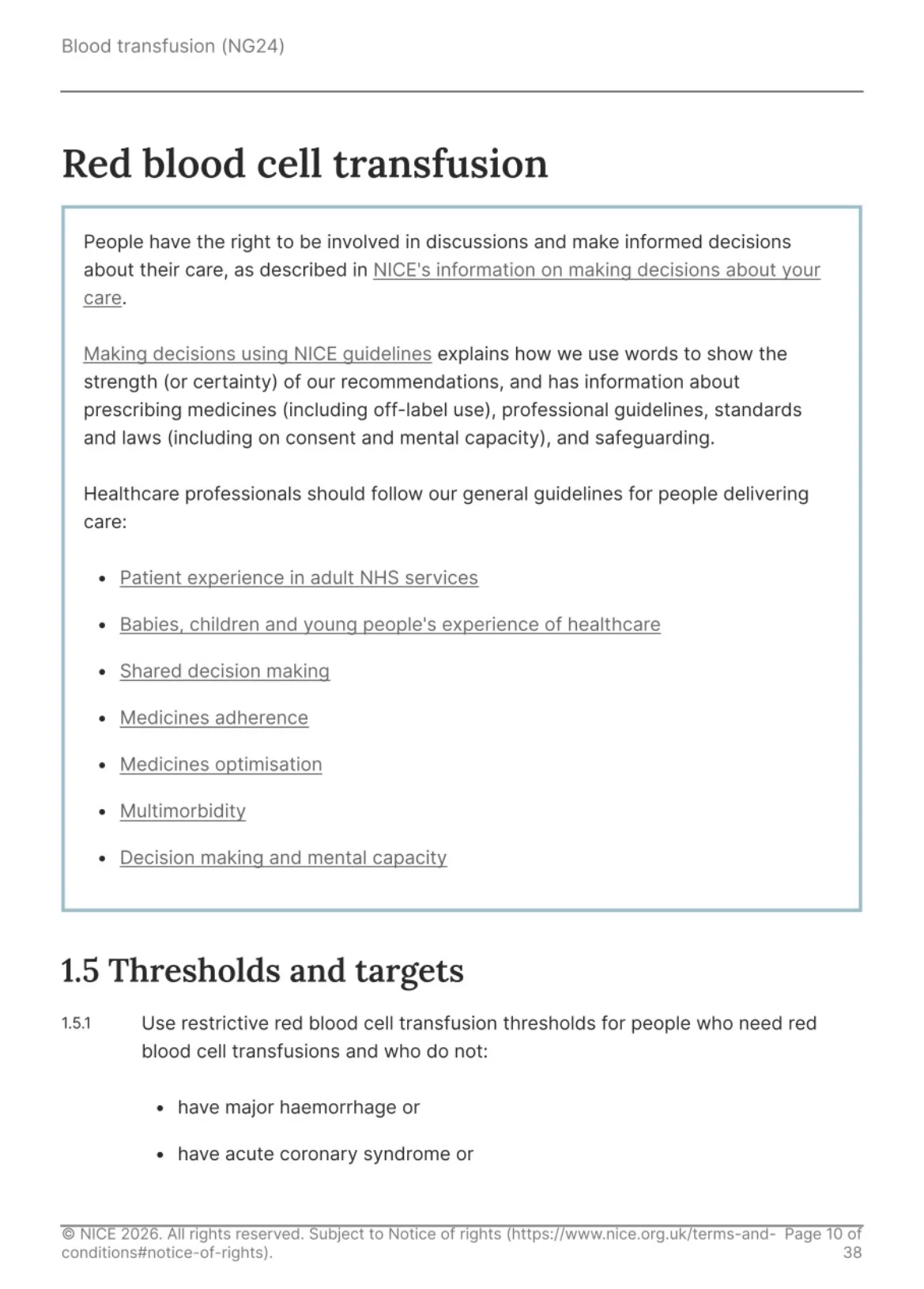
2. Red Blood Cell (RBC) Transfusion
Thresholds (Most Important Clinical Takeaway)
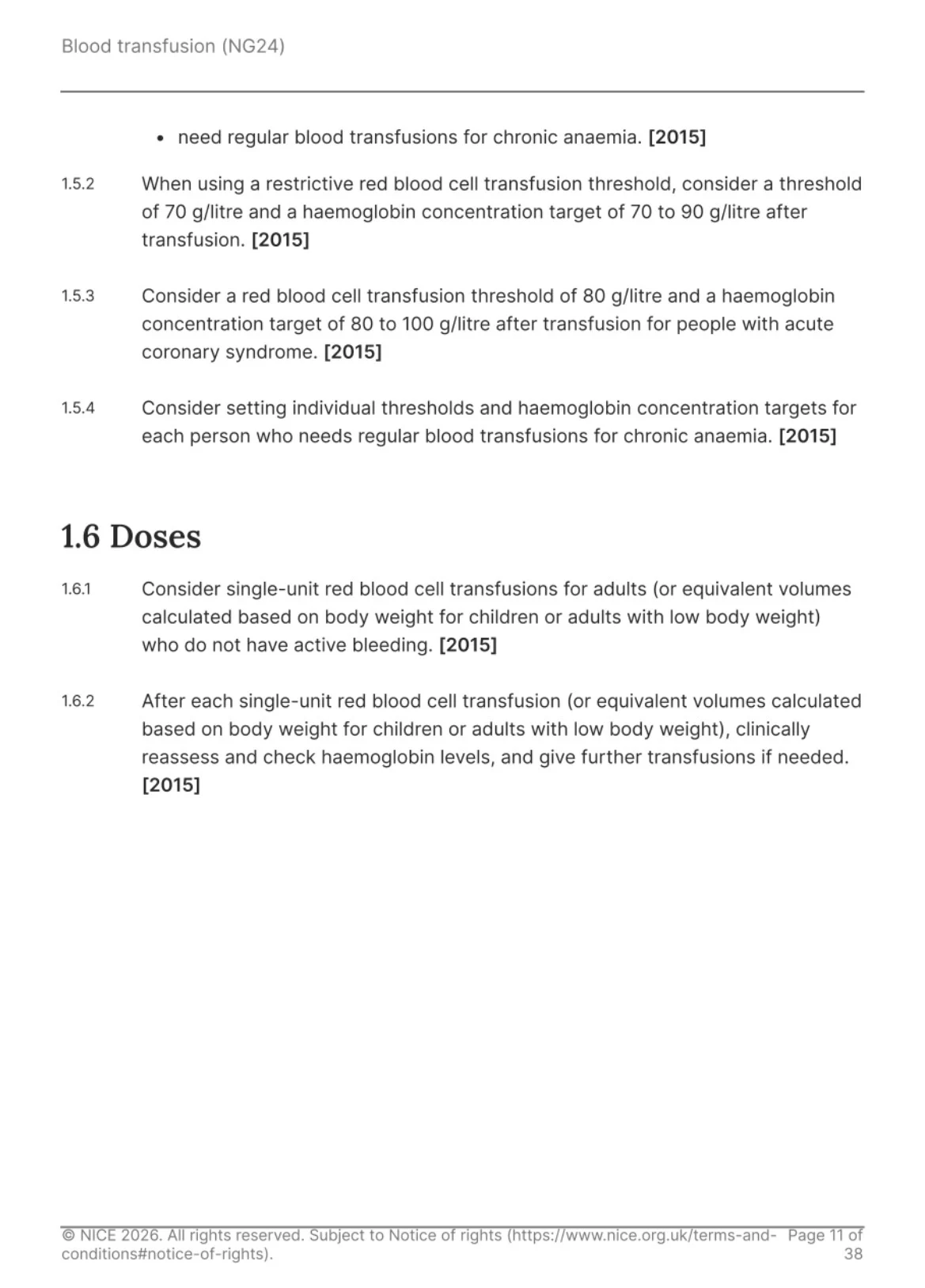
- Stable patients (no ACS, no major bleed):Hb trigger: ≤7 g/dL/ Target: 7–9 g/dL
- Acute Coronary Syndrome (ACS):Hb trigger: ≤8 g/dL/ Target: 8–10 g/dL
Dosing Strategy:
- Give 1 unit at a time
- Reassess clinically and Hb before next unit
This is critical to avoid over-transfusion
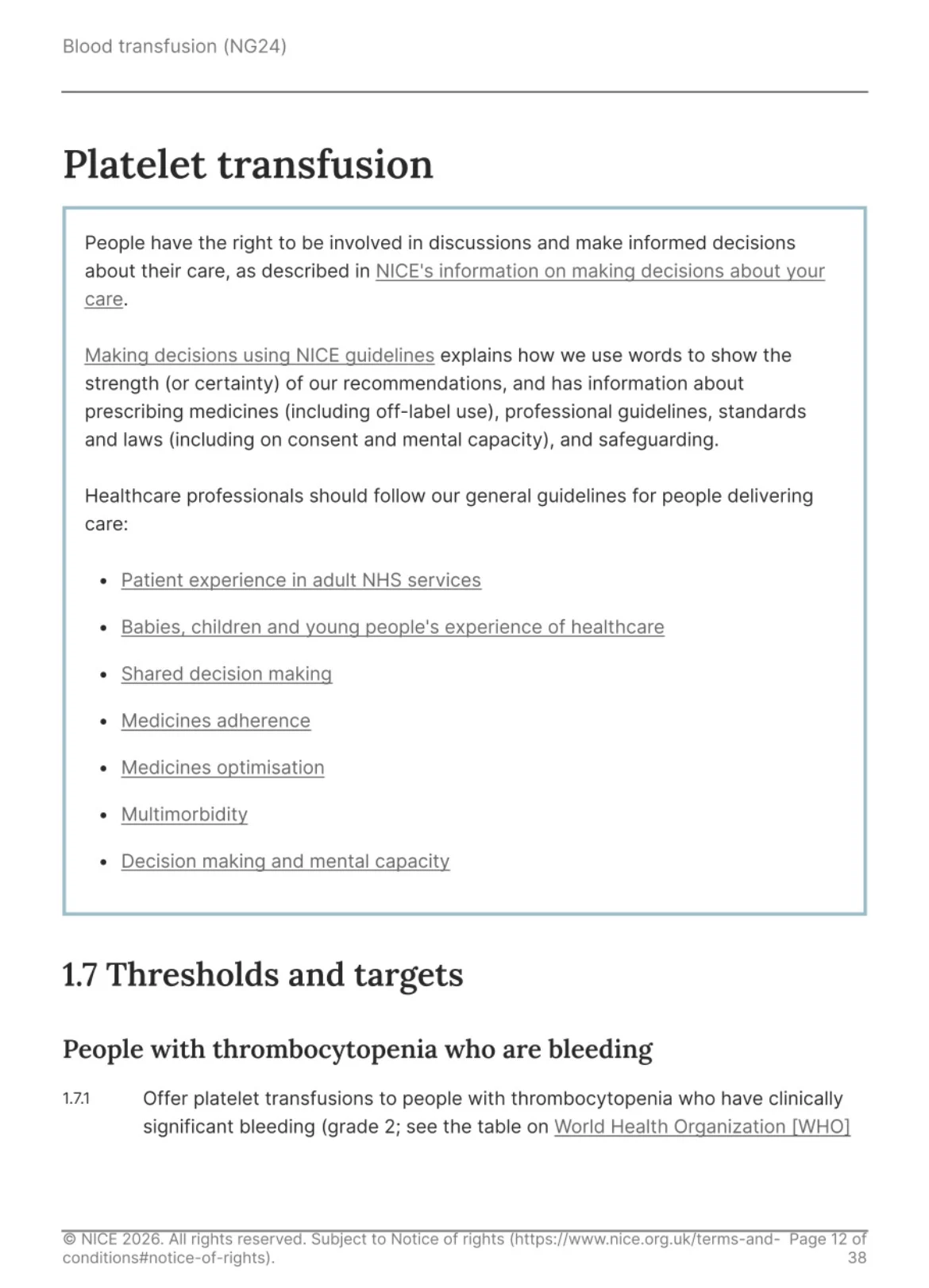
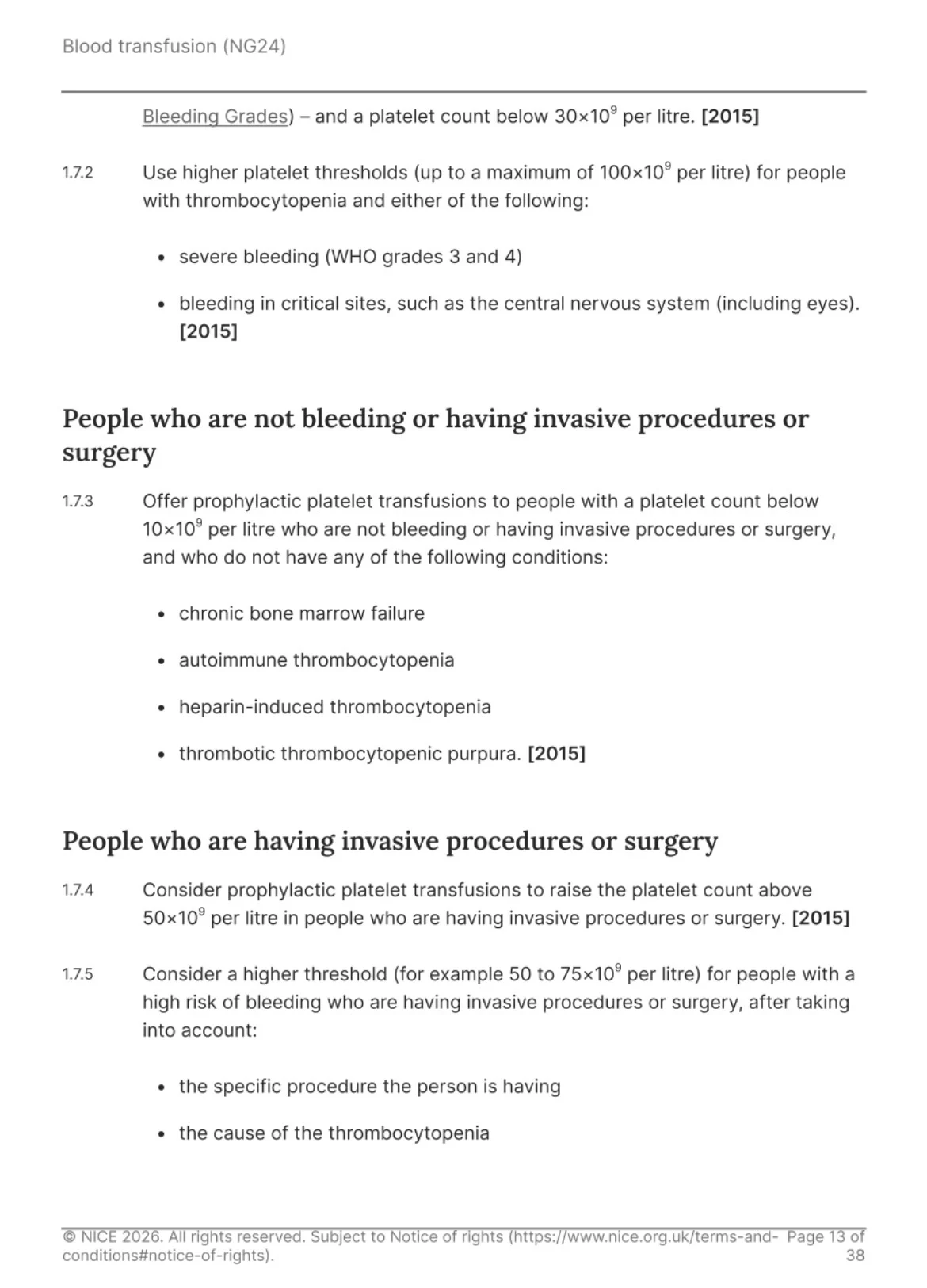
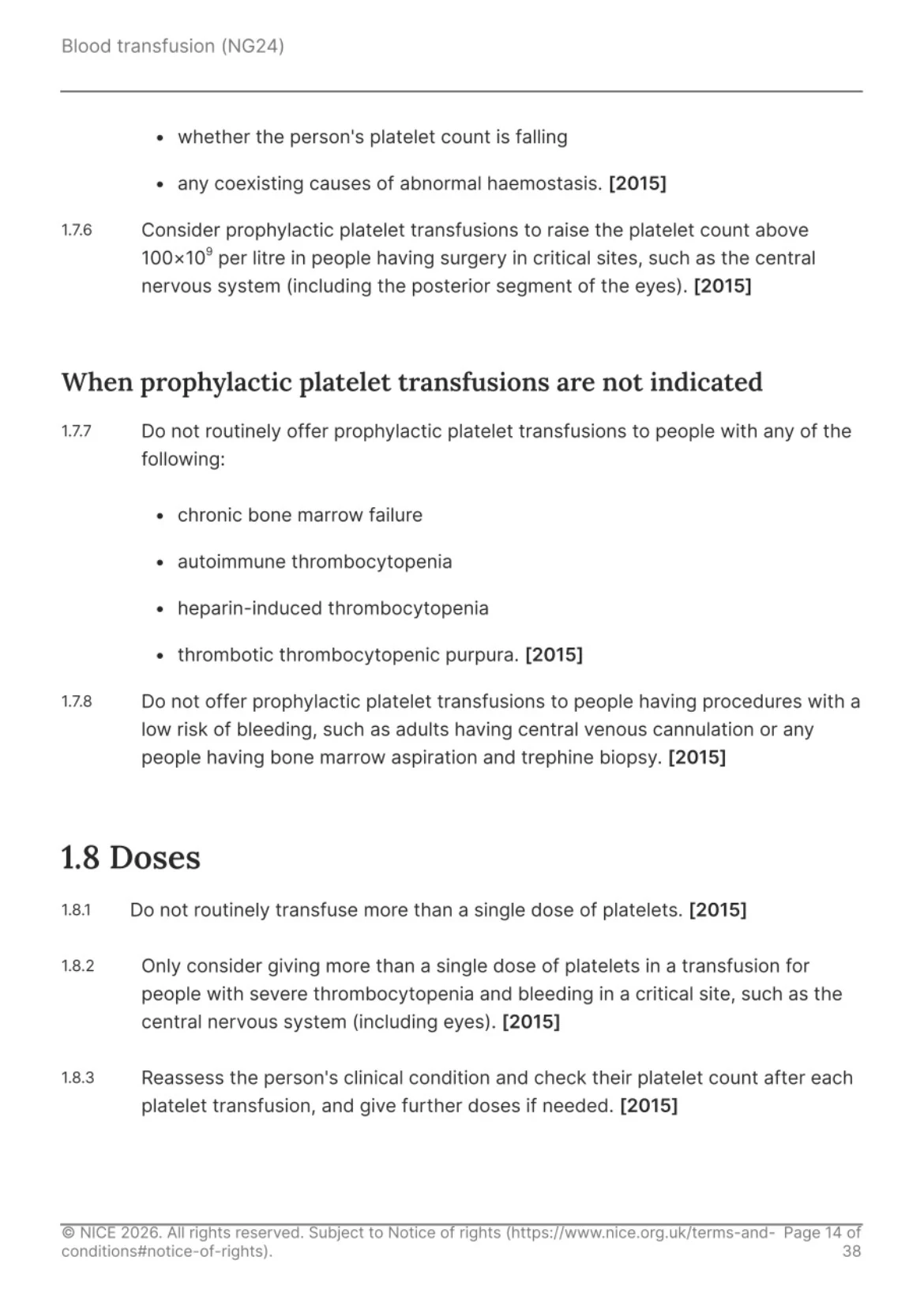
3. Platelet Transfusion
When Bleeding
- Platelets less than 30,000: Transfuse
- Severe bleeding / CNS bleed: target up to 100,000
Prophylaxis (No bleeding)
Lesser than 10,000: Transfuse
Procedures
- General surgery: greater than 50,000
- High-risk / CNS: greater than 100,000
Avoid Prophylaxis in: ITP HIT TTP
Chronic marrow failure (routine use not advised)
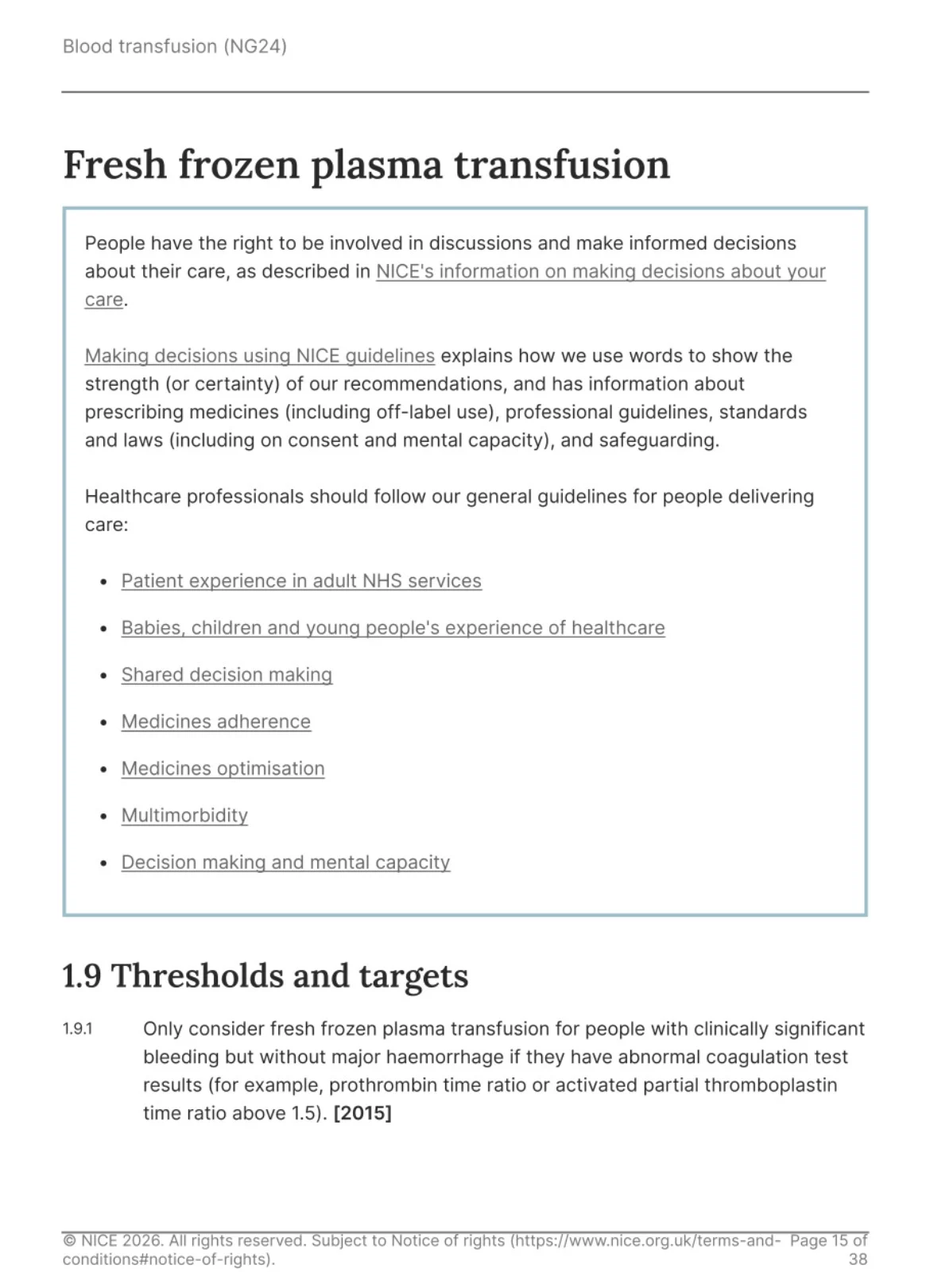
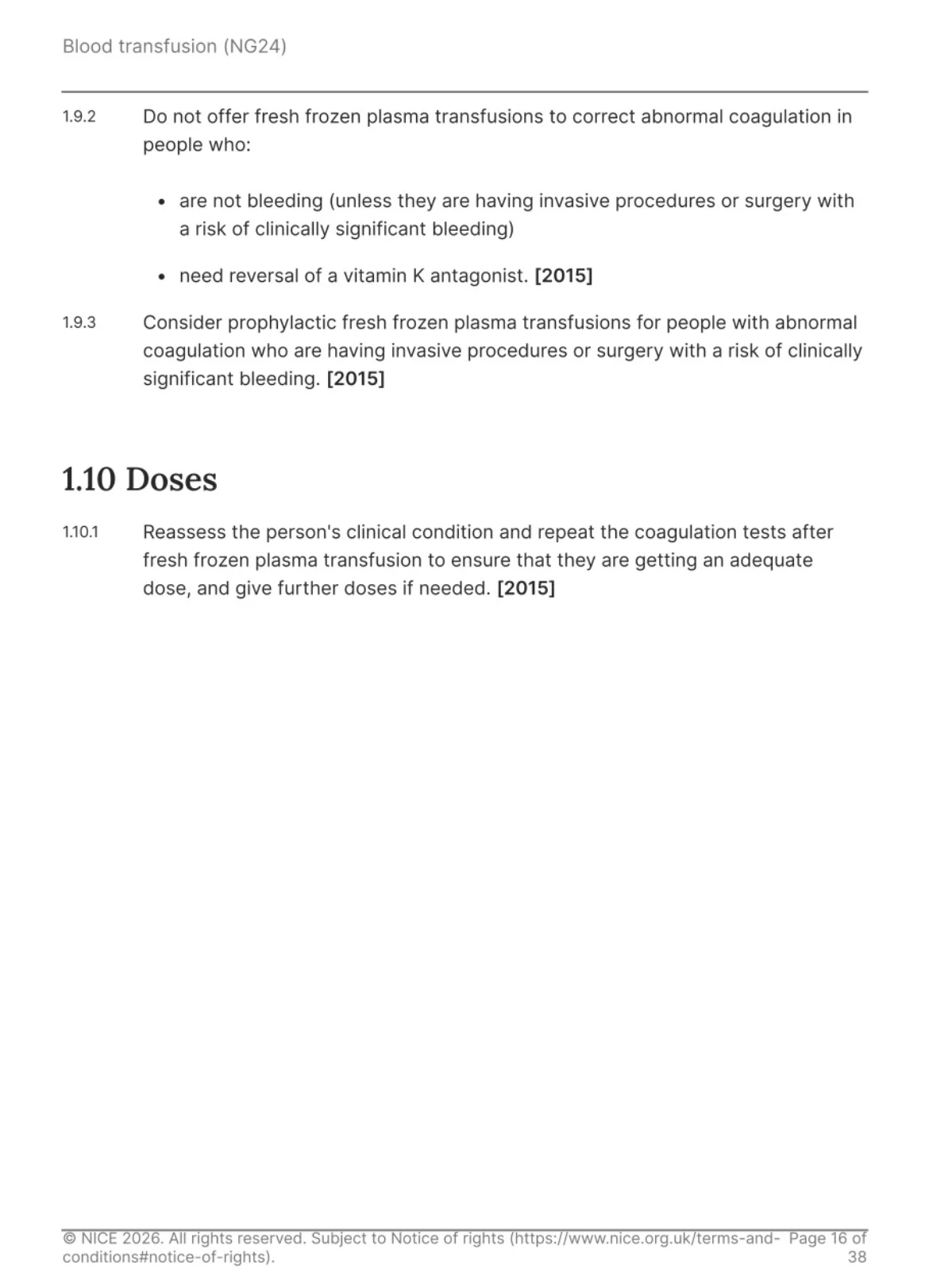
4. Fresh Frozen Plasma (FFP)
Indications
Active bleeding with INR/APTT greater than 1.5
Do NOT use:
- For abnormal INR without bleeding
- For warfarin reversal (use PCC instead)
Procedures
Consider if there is abnormal coagulation with bleeding risk
5. Cryoprecipitate
Indications
Bleeding with fibrinogen less than 1.5 g/L
Surgery:
If fibrinogen is less than 1.0 g/L, give prophylactically
Avoid:
If not bleeding and no procedure
6. Prothrombin Complex Concentrate (PCC)
Emergency Use
- Warfarin reversal in Severe bleeding
- Head injury with suspected ICH
- Monitor INR and repeat if needed
7. Tranexamic Acid (MAJOR 2026 UPDATE)
Practice-Changing Recommendation
Give TXA to ALL surgical patients if:
- Any bleeding risk
- Skin/mucosa breached
Dose:
Adults: 1 g IV before surgery
Benefits:
- Reduced Transfusion need
- Reduced Hospital stay
- Reduced Infection, bleeding
Caution:
Renal impairment with accumulation risk
Avoid wrong route (fatal if intrathecal)
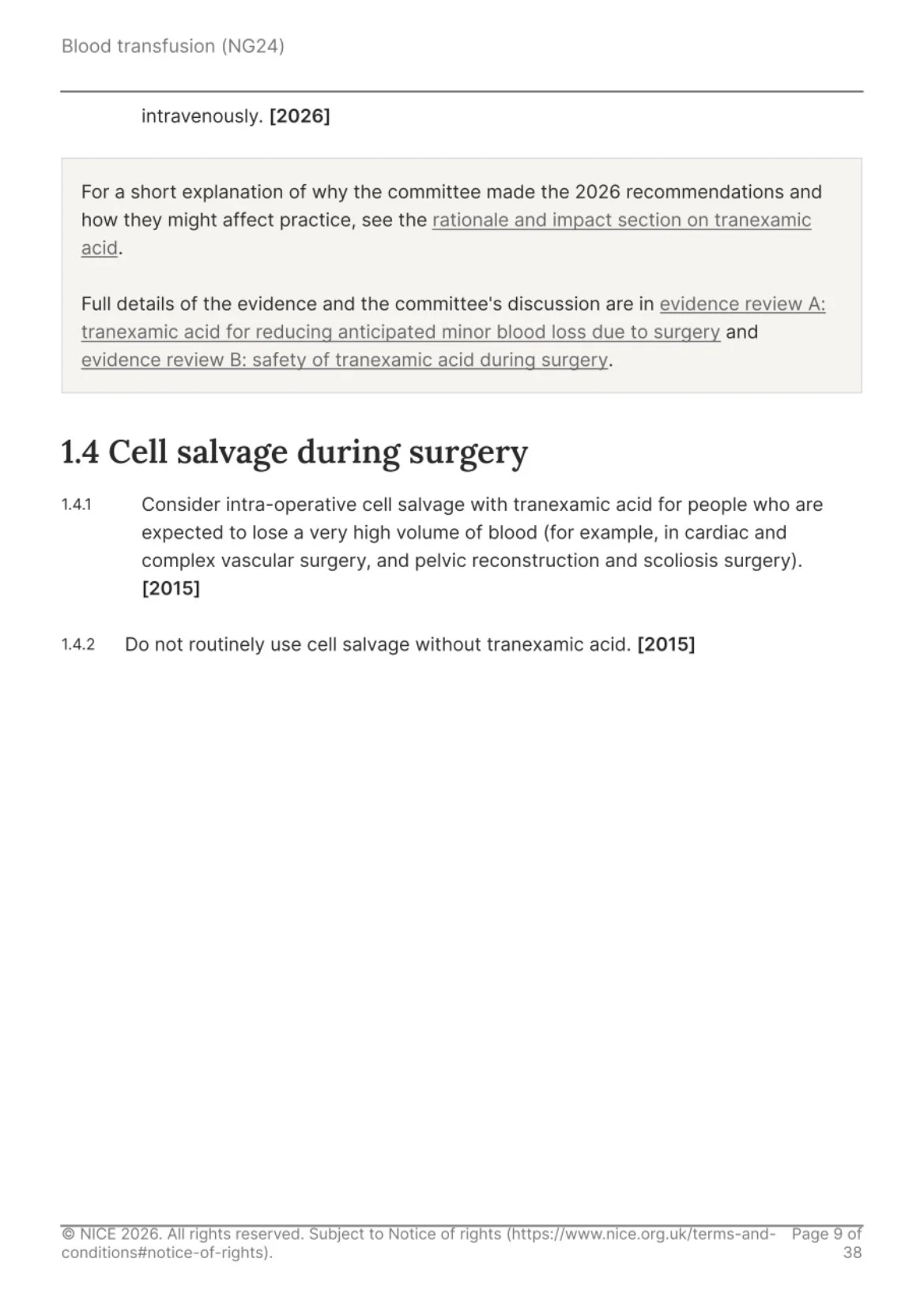
8. Reducing Need for Transfusion (Prevention Strategy)
Before Surgery
- Oral iron is first line
- IV iron is used if there is Intolerance, Short time to surgery
- Erythropoietin is not routine
Intra-op:
TXA with consideration of cell salvage for major blood loss
9. Safety and Monitoring
- Mandatory: Monitor Vitals before, during, after
- Watch for: Acute transfusion reactions
- System-level: Use electronic ID systems to reduce errors
10. Clinical ‘Rules of Thumb’:
- ‘7 is safe’ means Hb 7 g/dL in stable patients
- ‘One unit than reassess’
- Platelets:
10k (no bleed), 30k (bleed), 50k (surgery), 100k (CNS) - FFP only if bleeding and INR greater than 1.5
- Cryo if fibrinogen less than 1.5 and bleeding
- PCC equals warfarin emergency reversal
- TXA now routine in surgery
Source:
NICE Blood Transfusion Guideline (NG24, Updated February 2026)”

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 23, 2026, 20:46Grace Choung: A Novel CFHR5 Copy Number Variant in Postpartum Atypical HUS
-
Jul 23, 2026, 20:10Mohammad Alzoubi: One Month of Dual Antithrombotic Therapy After PCI Was Non-Inferior to 12 Months
-
Jul 23, 2026, 20:08Ahmed Bennis: Calcitriol Replenishment May Mitigate Ischemic Risk in MASLD
-
Jul 23, 2026, 20:06Mitsuaki Sawano: Can Cardiovascular Risk Prediction Models Developed in One Population be Reliably Applied to Another?
-
Jul 23, 2026, 20:05Abdul Muqtadir Abbasi: Hemostasis Isn’t About Memorizing Factor Numbers – It’s About Recognizing Patterns
-
Jul 23, 2026, 19:40Maureen Macharia: How Apixaban Transformed Modern Anticoagulation
-
Jul 23, 2026, 19:30Jordan Agay: Why We Need to Track the Neurological Costs of Anemia
-
Jul 23, 2026, 19:25William Archibald: Key Takeaways on VTE Cost-Effectiveness and Cancer Associated Thrombosis from ISTH 2026
-
Jul 23, 2026, 19:17Diego López Santos: Donation after Donation, I Just Reached 100