
AI generated
Apr 8, 2026, 14:17
Chokri Ben Lamine: Anticoagulation Switching Pearls
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
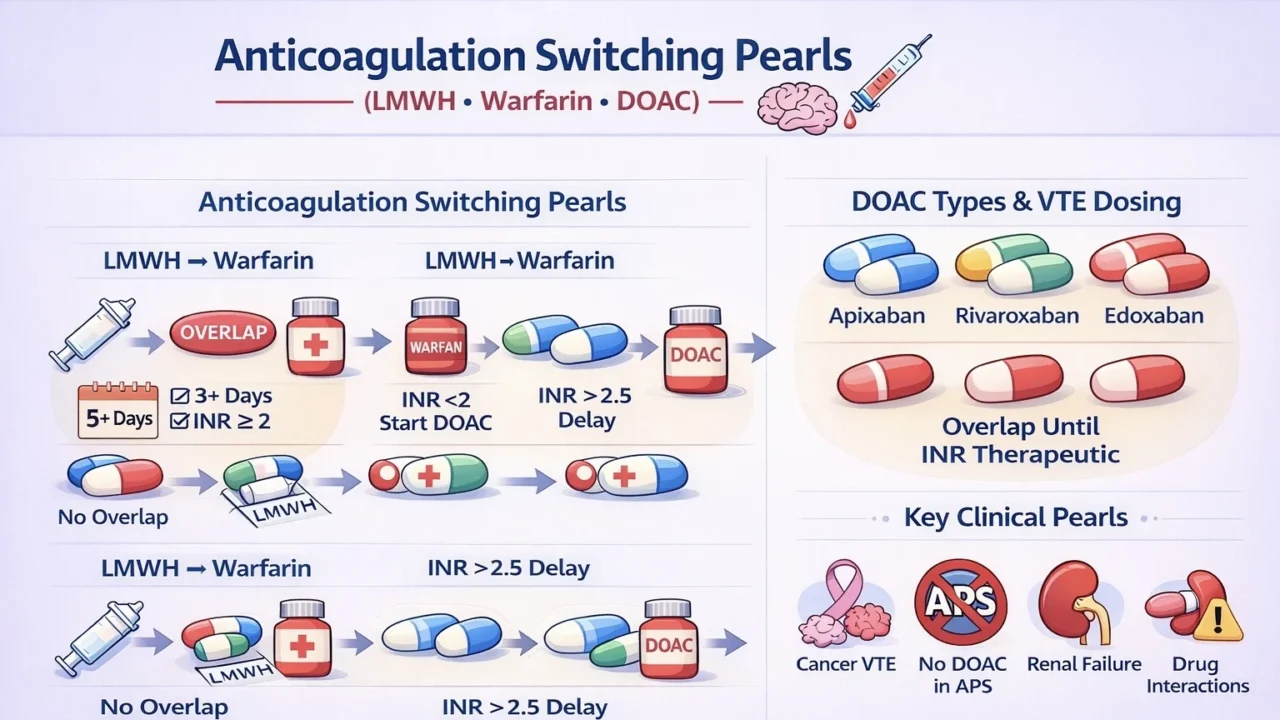
“Anticoagulation Switching Pearls (LMWH to Warfarin to DOAC)
LMWH to Warfarin – Overlap is mandatory:
- At least 5 days and INR at least 2 for 24–48 hours
- Prevent early hypercoagulability (decreased Protein C)
Start warfarin at 2–5 mg, adjust according to INR
Stop LMWH only when INR is stable and therapeutic
LMWH and DOAC
- Switching from LMWH to DOAC: Start DOAC at the time of the next LMWH dose; no overlap
- Switching from DOAC to LMWH: Start LMWH at the time of the next DOAC dose; no overlap
Warfarin to DOAC
- If INR is less than 2, start DOAC immediately
- If INR is 2 to 2.5, start on the same day
- If INR is greater than 2.5, delay
DOAC to Warfarin
- Overlap DOAC with warfarin
- Stop DOAC once INR is therapeutic
DOAC VTE Dosing in Adults
Apixaban
- Acute VTE: 10 mg BID for 7 days
- Then 5 mg BID
- Extended 2.5 mg BID
- Least bleeding risk, preferred in many hematology patients
Rivaroxaban
- Acute VTE: 15 mg BID for 21 days
- Then 20 mg once daily
- Extended 10 mg once daily
- Take with food
Edoxaban
- Requires lead-in LMWH for 5 to 10 days
- Then 60 mg once daily
- Reduce to 30 mg if weight 60 kg or less or CrCl 15 to 50
Dabigatran
- Requires LMWH lead-in for 5 to 10 days
- Then 150 mg BID
- Avoid if CrCl less than 30
- Higher gastrointestinal side effects
Key Clinical Pearls
- Only dabigatran and edoxaban need LMWH lead-in
- Apixaban and rivaroxaban follow a single-drug approach
Cancer-associated VTE
- DOAC such as apixaban or rivaroxaban preferred
- Use LMWH if gastrointestinal or genitourinary bleeding risk
APS triple positive
- Avoid DOAC; use warfarin
Renal failure
- Prefer warfarin if severe CKD
Drug interactions
- DOAC affected by P-gp and CYP3A4 inhibitors such as azole, chemotherapy, tyrosine kinase inhibitors
Bridging rule
- Warfarin requires overlap
- DOAC requires timing switch with no overlap.”
Stay updated with Hemostasis Today.
-
Jul 7, 2026, 23:20Balaji Balagani: Exploring Pulmonary Embolism
-
Jul 7, 2026, 23:03Roxana González Mazarío: The Phenotype-Specific Cardiovascular Risks in AAV
-
Jul 7, 2026, 22:52Harry Spoelstra: LongC0VID Still has Zero Proven Treatments
-
Jul 7, 2026, 22:39Satya K. Morar: Acute Portal Vein Thrombosis as an Exceptionally Rare Complication of Liver Biopsy in CVID
-
Jul 7, 2026, 22:23Aravind Palraj: Antiphospholipid Syndrome is not Just ‘Start Warfarin and Follow INR’
-
Jul 7, 2026, 20:59William Aird: An Unlucky Turn Into the Renal Artery
-
Jul 7, 2026, 20:58Chokri Ben Lamine: The Two-Hit Model of TRALI
-
Jul 7, 2026, 20:57New Issue of Blood Out Now – Blood Journals Portfolio
-
Jul 7, 2026, 20:56Priyadarshini Ramakrishnan: Schistocytes – The Most “Misleading Heroes” in a Peripheral Smear