
Chokri Ben Lamine: The Two-Hit Model of TRALI
Chokri Ben Lamine, Assistant Consultant at King Faisal Specialist Hospital and Research Center, shared a post on X:
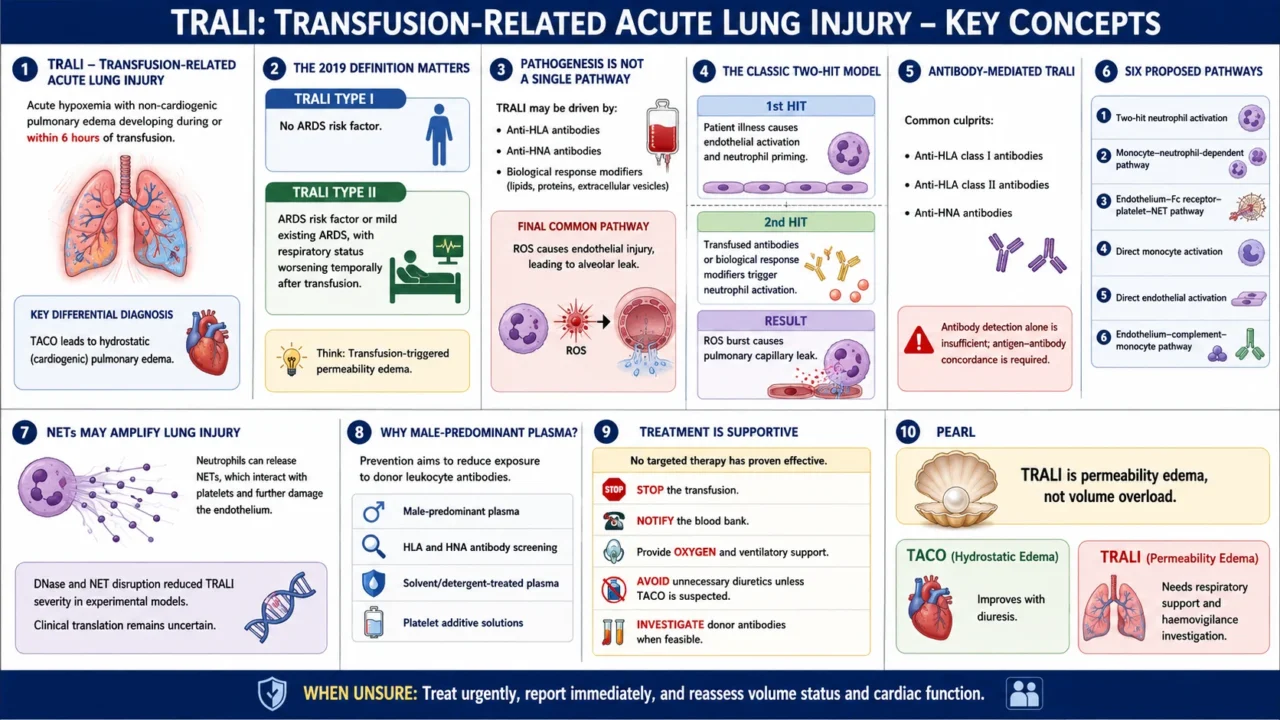
“1.TRALI – transfusion-related acute lung injury
Acute hypoxemia with non-cardiogenic pulmonary edema during or within 6h of transfusion.
Key DDx: TACO leads to hydrostatic and cardiogenic edema.
2.2019 definition matters
- TRALI type I: no ARDS risk factor
- TRALI type II: ARDS risk factor or mild ARDS, but respiratory status worsens temporally after transfusion.
Think ‘transfusion-triggered permeability edema.’
3.Pathogenesis is not one pathway
TRALI may be driven by:
- anti-HLA and anti-HNA antibodies
- biological response modifiers: lipids, proteins, extracellular vesicles
Final common pathway: ROS causes endothelial injury, leading to alveolar leak..
4.Classic 2-hit model
- 1st hit: patient illness causes endothelial activation and neutrophil priming
- 2nd hit: transfused antibodies or BRMs trigger neutrophil activation
Result: ROS burst causes pulmonary capillary leak
5.Antibody-mediated TRALI
Common culprits:
- anti-HLA class I
- anti-HLA class II
- anti-HNA antibodies
But antibody detection alone is not enough; need antigen–antibody concordance.
6.Six proposed pathways
- Two-hit neutrophil activation
- Monocyte with neutrophil dependent
- Endothelium–FcR–platelet–NET pathway
- Direct monocyte activation
- Direct endothelial activation
- Endothelium–complement–monocyte pathway
7.NETs may amplify injury
Neutrophils can release NETs, which interact with platelets and worsen endothelial damage.
DNase and NET-disruption reduced TRALI severity in experimental models.
Clinical translation still uncertain.
8.Why male-predominant plasma?
Prevention aims to reduce exposure to donor leukocyte antibodies.
Strategies include:
- male-predominant plasma
- HLA and HNA antibody screening
- solvent or detergent plasma
- platelet additive solutions
9.Treatment is supportive
No proven targeted therapy yet.
Practical approach:
- stop transfusion
- notify blood bank
- oxygen and ventilatory support
- avoid unnecessary diuretics unless TACO possible
- investigate donor antibodies when feasible
10.Pearl
- TRALI is permeability edema, not volume overload.
- TACO improves with diuresis; TRALI needs respiratory support and haemovigilance investigation.
- When unsure: treat urgently, report immediately, and reassess volume and cardiac status.”
Other posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jul 7, 2026, 20:59William Aird: An Unlucky Turn Into the Renal Artery
-
Jul 7, 2026, 20:57New Issue of Blood Out Now – Blood Journals Portfolio
-
Jul 7, 2026, 20:56Priyadarshini Ramakrishnan: Schistocytes – The Most “Misleading Heroes” in a Peripheral Smear
-
Jul 7, 2026, 20:55Natasa Blagojevic-Stokic: Exploring the Role of ATP and Calcium Homeostasis in Autism
-
Jul 7, 2026, 17:49Alan Nurden: Safer Antithrombotic Therapy Through GPVI
-
Jul 7, 2026, 17:29Anticoagulation Reversal in 2026: Are We Winning the Bleeding Battle? – Francisco Chacón-Lozsán
-
Jul 7, 2026, 17:25Jim Hoffman: Targeting NETosis to Restore Immune Homeostasis
-
Jul 7, 2026, 17:14Shabneez Hussain: Blood Transfusion Professionals Connecting at ISBT 2026
-
Jul 7, 2026, 17:04Mariam Swidan: Vitamin B12 Deficiency and the Hidden Risk of Neurological Damage