
Apr 1, 2026, 17:15
Chokri Ben Lamine: Differentiating Reactive from Clonal Causes in Adult Neutrophilia
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
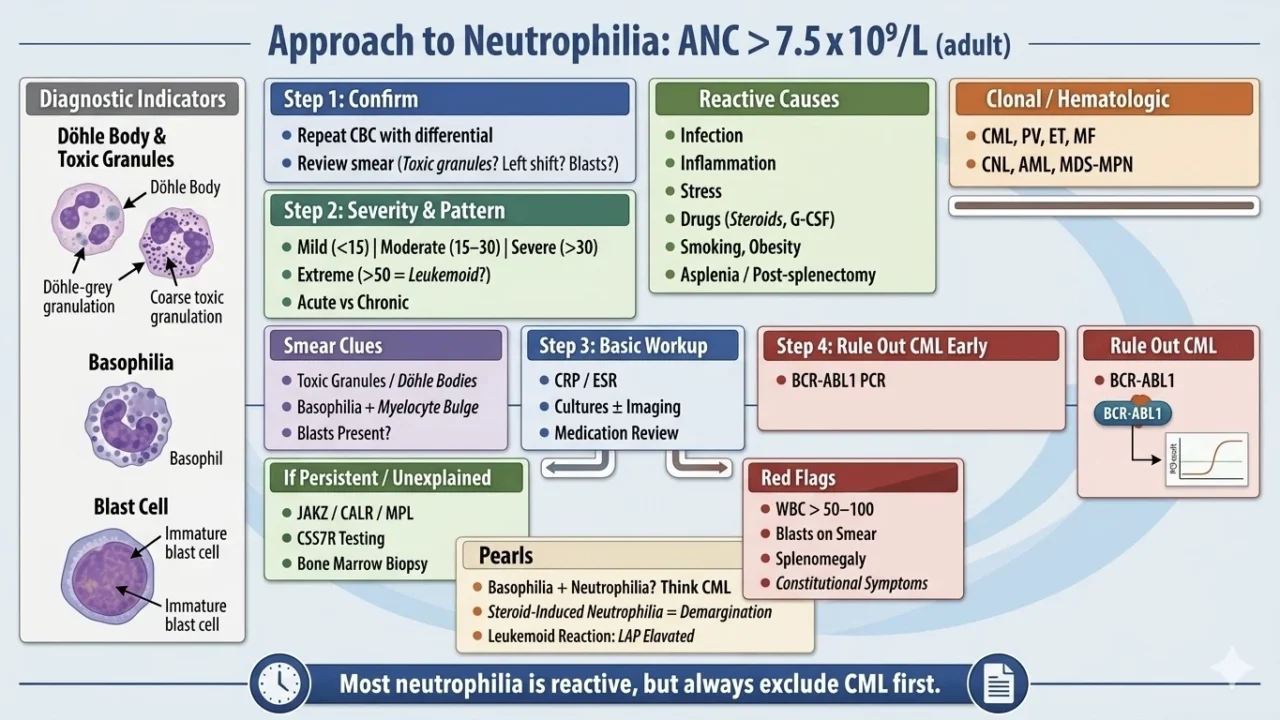
“Neutrophilia approach: ANC greater than 7.5 ×10⁹/L (adult) should be classified reactive vs clonal
Step 1: confirm
- repeat CBC with differential
- review smear (toxic granulation? left shift? blasts?)
Step 2: severity and pattern
- mild (<15) | moderate (15–30) | severe (>30) | extreme (>50 = leukemoid?)
- acute vs chronic
Reactive causes (most common)
- infection (bacterial, severe viral early)
- inflammation (RA, IBD, vasculitis)
- stress (trauma, surgery, MI)
- drugs (steroids, G-CSF, lithium)
- smoking, obesity
- asplenia/post-splenectomy
Clonal / hematologic
- MPN: CML, PV, ET, MF
- CNL (rare, CSF3R+)
- AML with leukocytosis
- MDS/MPN overlap
Smear clues
- toxic granulation/Döhle bodies indicates a reactive
- basophilia with myelocyte bulge then think CML
- blasts raise concern for acute leukemia
Step 3: basic workup
- CRP/ESR
- cultures ± imaging if infection suspected
- medication review
Step 4: rule out CML early
BCR-ABL1 PCR (must not miss)
If persistent/unexplained
- JAK2 / CALR / MPL
- CSF3R if CNL suspected
- bone marrow biopsy
Red flags (urgent)
- WBC greater than 50–100
- blasts on smear
- organomegaly
- constitutional symptoms
Pearls
- neutrophilia with basophilia should be considered CML until proven otherwise
- steroid-induced neutrophilia results from demargination (no left shift)
- leukemoid reaction can mimic leukemia but LAP high
One-liner
most neutrophilia is reactive, but always exclude CML first”
Stay updated with Hemostasis Today.
-
Jul 8, 2026, 21:30Matthew Gouveia: How VNS-REHAB Is Transforming the Future of Stroke Rehabilitation
-
Jul 8, 2026, 21:22What Hundreds of Stroke Stories Have Taught Diana Kerr About Recovery and Resilience – Stroke Foundation
-
Jul 8, 2026, 19:50Heghine Khachatryan: Why the EHC Fully Supports the Lancet Commission on Women’s Hematological Health
-
Jul 8, 2026, 19:40Autoregulation Failure in SVD and Cognitive Impairment – International Journal of Stroke
-
Jul 8, 2026, 19:30Ahmed Mostafa: Why Antibodies Cause Organ Rejection
-
Jul 8, 2026, 19:28Erika Bocanegra: Witnessing 25 Years of Progress in Bleeding Disorders Care
-
Jul 8, 2026, 19:27Ahmadou Ouedraogo: Do You Know Your Blood Type?
-
Jul 8, 2026, 19:26Javed Anees: An Evidence-Based Clinical Guide to ESA Therapy
-
Jul 8, 2026, 19:25Paul Breillat: Nature Reviews Rheumatology Highlights Our VEXAS Syndrome Research